How to Read Fetal Non Stress Test Uterin Contractions Above 120
What is cardiotocography?
Cardiotocography (CTG) is used during pregnancy to monitor fetal middle rate and uterine contractions. It is almost commonly used in the tertiary trimester and its purpose is to monitor fetal well-being and allow early detection of fetal distress. An abnormal CTG may indicate the need for further investigations and potential intervention.
Check out our CTG quiz on the Geeky Medics quiz platform to put your CTG interpretation knowledge to the exam.
How CTG works
The device used in cardiotocography is known as a cardiotocograph. It involves the placement of 2 transducers onto the abdomen of a pregnant woman. Ane transducer records the fetal heart rate using ultrasound and the other transducer monitors the contractions of the uterus by measuring the tension of the maternal abdominal wall (providing an indirect indication of intrauterine pressure). The CTG is then assessed past a midwife and the obstetric medical team.
How to read a CTG
To interpret a CTG y'all demand a structured method of assessing its various characteristics. The most popular structure can be remembered using the acronym DR C BRAVADO:
- DR: Define take a chance
- C: Contractions
- BRa: Baseline rate
- 5: Variability
- A: Accelerations
- D: Decelerations
- O: Overall impression
Y'all might also exist interested in our OSCE Flashcard Collection which contains over 2000 flashcards that comprehend clinical exam, procedures, communication skills and data interpretation.
Define risk
When performing CTG interpretation, y'all kickoff demand to determine if the pregnancy is loftier or low hazard. This is important every bit it gives more context to the CTG reading (east.g. if the pregnancy categorised as high-risk, the threshold for intervention may be lower). Some reasons a pregnancy may be considered high gamble are shown below.1
Maternal medical illness
- Gestational diabetes
- Hypertension
- Asthma
Obstetric complications
- Multiple gestation
- Postal service-date gestation
- Previous cesarean department
- Intrauterine growth brake
- Premature rupture of membranes
- Built malformations
- Oxytocin induction/augmentation of labour
- Pre-eclampsia
Other risk factors
- Absence of prenatal care
- Smoking
- Drug abuse
Contractions
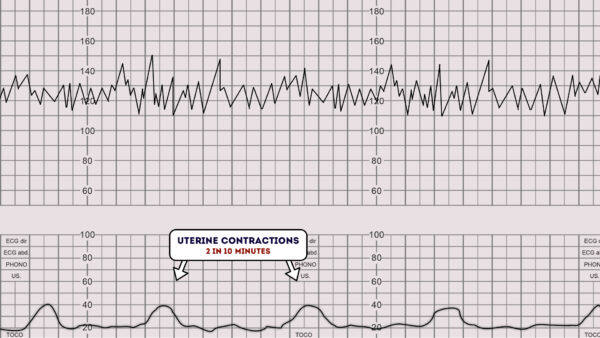
Next, you lot need to record the number of contractions nowadays in a ten minute menstruation.
Each big square on the example CTG chart below is equal toi minute, and so look at how many contractions occurred within 10 big squares.
Individual contractions are seen as peaks on the part of the CTG monitoring uterine action.
Assess contractions for the following:
- Duration: How long do the contractions last?
- Intensity: How strong are the contractions (assessed using palpation)?
- In the below example, there are ii contractions in a 10 minute catamenia (this is ofttimes referred to every bit "2 in 10").
Baseline rate of the fetal centre
The baseline rate is the average heart rate of the fetus within a ten-infinitesimal window.
Look at the CTG and assess what the average center rate has been over the last 10 minutes, ignoring any accelerations or decelerations.
A normal fetal centre rate is between 110-160 bpm.

Fetal tachycardia
Fetal tachycardia is divers every bit a baseline heart rate greater than 160 bpm.
Causes of fetal tachycardia include:
- Fetal hypoxia
- Chorioamnionitis
- Hyperthyroidism
- Fetal or maternal anaemia
- Fetal tachyarrhythmia
Fetal bradycardia
Fetal bradycardia is defined equally a baseline centre rate of less than 100 bpm.
It is common to accept a baseline center rate of between 100-120 bpm in the following situations:
- Postdate gestation
- Occiput posterior or transverse presentations
Astringent prolonged bradycardia (less than 80 bpm for more than than 3 minutes) indicates astringent hypoxia.
Causes of prolonged severe bradycardia include:
- Prolonged string compression
- Cord prolapse
- Epidural and spinal anaesthesia
- Maternal seizures
- Rapid fetal descent
Variability
Baseline variability refers to the variation of fetal heart rate from 1 beat to the side by side.
Variability occurs as a result of the interaction between the nervous system, chemoreceptors, baroreceptors and cardiac responsiveness.
It is, therefore, a good indicator of how healthy a fetus is at that particular moment in time, as a healthy fetus will constantly be adapting its heart rate in response to changes in its environment.
Normal variability indicates an intact neurological organisation in the fetus.
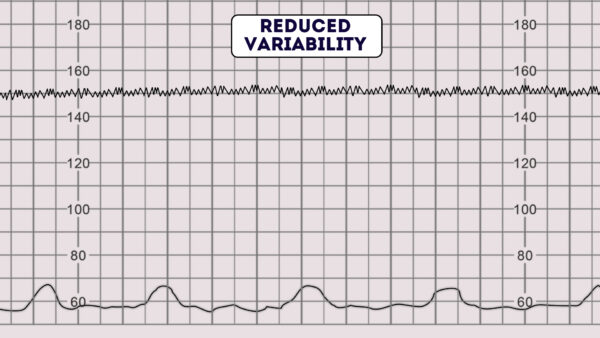
Normal variability is between 5-25 bpm.three
To calculate variability you need to assess how much the peaks and troughs of the heart rate deviate from the baseline rate (in bpm).
Variability categorisation
Variability can be categorised equally either reassuring, not-reassuring or abnormal. three
Reassuring: 5 – 25 bpm
Non-reassuring:
- less than v bpm for betwixt thirty-50 minutes
- more than 25 bpm for xv-25 minutes
Abnormal:
- less than 5 bpm for more than than l minutes
- more than 25 bpm for more than than 25 minutes
- sinusoidal

Reduced variability tin be caused past any of the following:2
- Fetal sleeping: this should last no longer than 40 minutes (this is the most mutual cause)
- Fetal acidosis (due to hypoxia): more probable if tardily decelerations are too nowadays
- Fetal tachycardia
- Drugs: opiates, benzodiazepines, methyldopa and magnesium sulphate
- Prematurity: variability is reduced at earlier gestation (<28 weeks)
- Congenital centre abnormalities
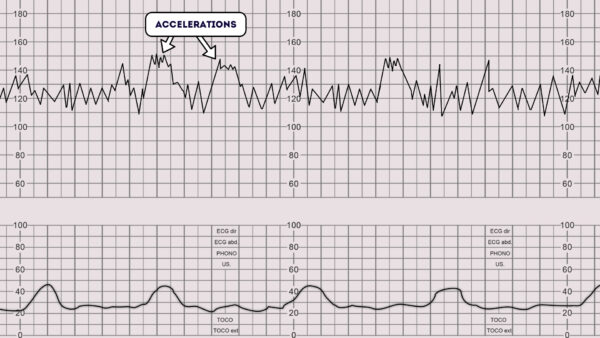
Accelerations
Accelerations are an abrupt increase in the baseline fetal center charge per unit of greater than 15 bpm for greater than 15 seconds.1
The presence of accelerations is reassuring.
Accelerations occurring alongside uterine contractions is a sign of a good for you fetus.
The absence of accelerations with an otherwise normal CTG is of uncertain significance.
Decelerations
Decelerations are an sharp decrease in the baseline fetal heart rate of greater than fifteen bpm for greater than 15 seconds.
The fetal heart rate is controlled past the autonomic and somatic nervous system. In response to hypoxic stress, the fetus reduces its center charge per unit to preserve myocardial oxygenation and perfusion. Dissimilar an adult, a fetus cannot increase its respiration depth and rate. This reduction in heart rate to reduce myocardial demand is referred to every bit a deceleration.
In that location are a number of different types of decelerations, each with varying significance.
Early deceleration
Early decelerations start when the uterine wrinkle begins and recover when uterine contraction stops. This is due to increased fetal intracranial force per unit area causing increased vagal tone. It therefore quickly resolves in one case the uterine wrinkle ends and intracranial pressure reduces. This type of deceleration is, therefore, considered to be physiological and not pathological.3

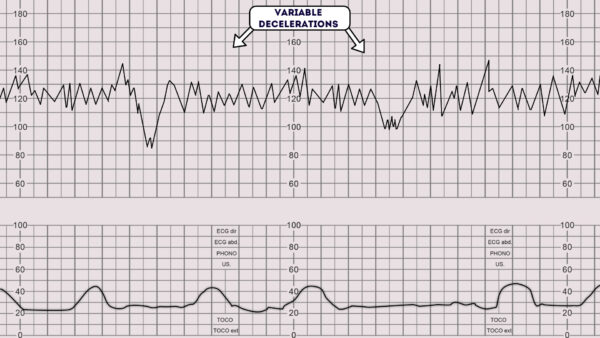
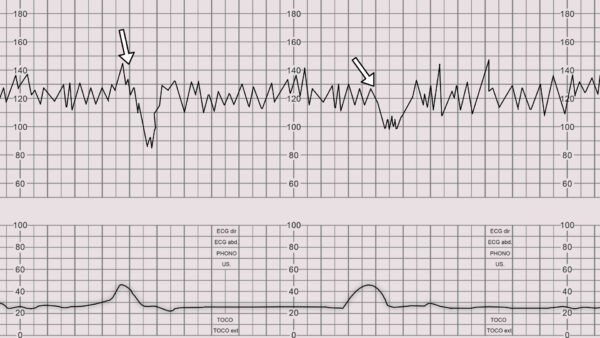
Variable deceleration
Variable decelerations are observed as a rapid fall in baseline fetal middle rate with a variable recovery phase.
They are variable in their duration and may not have whatsoever human relationship to uterine contractions.
They are virtually oftentimes seen during labour and in patients' with reduced amniotic fluid book.
All fetuses experience stress during the labour process, as a result of uterine contractions reducing fetal perfusion. Whilst fetal stress is to exist expected during labour, the claiming is to pick upward pathological fetal distress.
Variable decelerations are usually caused by umbilical cord compression. The machinery is as follows:one
1. The umbilical vein is ofttimes occluded beginning causing an dispatch of the fetal eye rate in response.
2. Then the umbilical artery is occluded causing a subsequent rapid deceleration.
three. When pressure level on the cord is reduced another acceleration occurs and and so the baseline rate returns.
The accelerations before and after a variable deceleration are known as the shoulders of deceleration. Their presence indicates the fetus is not yet hypoxic and is adapting to the reduced claret menstruum. Variable decelerations can sometimes resolve if the mother changes position. The presence of persistent variable decelerations indicates the need for close monitoring. Variable decelerations without the shoulders are more worrying, equally it suggests the fetus is becoming hypoxic.
Tardily deceleration
Late decelerations brainstorm at the summit of the uterine contraction and recover after the contraction ends. This type of deceleration indicates there is insufficient blood period to the uterus and placenta. As a result, blood flow to the fetus is significantly reduced causing fetal hypoxia and acidosis.
Causes of reduced uteroplacental blood menstruum include:ane
- Maternal hypotension
- Pre-eclampsia
- Uterine hyperstimulation
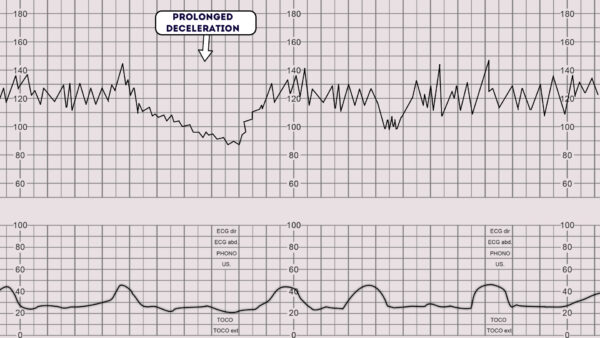
Prolonged deceleration
A prolonged deceleration is defined as a deceleration that lasts more than 2 minutes:
- If it lasts between ii-3 minutes it is classed equally non-reassuring.
- If it lasts longer than 3 minutes information technology is immediately classed as abnormal.
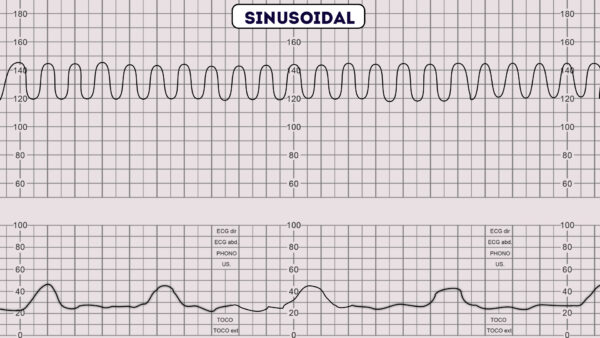
Sinusoidal pattern
A sinusoidal CTG design is rare, however, if present it is very concerning as information technology is associated with high rates of fetal morbidity and mortality.one
A sinusoidal CTG design has the post-obit characteristics:
- A smooth, regular, moving ridge-like pattern
- Frequency of around 2-5 cycles a minute
- Stable baseline rate around 120-160bpm
- No beat to beat variability
A sinusoidal blueprint usually indicates 1 or more of the post-obit:
- Astringent fetal hypoxia
- Severe fetal anaemia
- Fetal/maternal haemorrhage
Overall impression
Once you have assessed all aspects of the CTG you need to decide your overall impression.
The overall impression can be described equally either reassuring, suspicious or abnormal.3
Overall impression is determined past how many of the CTG features were either reassuring, not-reassuring or abnormal. The NICE guidelines below demonstrate how to decide which category a CTG falls into.3
Reassuring
Baseline centre charge per unit
- 110 to 160 bpm
Baseline variability
- v to 25 bpm
Decelerations
- None or early on
- Variable decelerations with no apropos characteristics for less than 90 minutes
Not-reassuring
Baseline centre charge per unit
Either of the below would be classed as non-reassuring:
- 100 to 109 bpm
- 161 to 180 bpm
Baseline variability
Either of the below would be classed as non-reassuring:
- Less than v for 30 to fifty minutes
- More 25 for xv to 25 minutes
Decelerations
Any of the below would be classed as non-reassuring:
- Variable decelerations with no concerning characteristics for xc minutes or more.
- Variable decelerations with any apropos characteristics in upward to 50% of contractions for 30 minutes or more.
- Variable decelerations with any apropos characteristics in over l% of contractions for less than xxx minutes.
- Tardily decelerations in over 50% of contractions for less than 30 minutes, with no maternal or fetal clinical risk factors such as vaginal bleeding or pregnant meconium.
Aberrant
Baseline heart charge per unit
Either of the below would exist classed as abnormal:
- Beneath 100 bpm
- To a higher place 180 bpm
Baseline variability
Whatsoever of the below would be classed as abnormal:
- Less than five for more than 50 minutes
- More than 25 for more than 25 minutes
- Sinusoidal
Decelerations
Any of the below would be classed as aberrant:
- Variable decelerations with any apropos characteristics in over 50% of contractions for xxx minutes (or less if any maternal or fetal clinical risk factors – see higher up).
- Late decelerations for 30 minutes (or less if any maternal or fetal clinical gamble factors).
- Astute bradycardia, or a unmarried prolonged deceleration lasting iii minutes or more than.
Regard the following as apropos characteristics of variable decelerations:
- Lasting more than 60 seconds
- Reduced baseline variability inside the deceleration
- Failure to render to baseline
- Biphasic (W) shape
- No shouldering
Reviewer
Dr Venkatesh Subramanian
Obstetrics & Gynaecology Registrar in London
References
- AMIR SWEHA, G.D. Interpretation of the Electronic Fetal Heart Charge per unit During Labor. Am Fam Physician. 1999 May 1;59(9):2487-2500. Bachelor from: [LINK].
- Clinical obstetrics and gynaecology. 2nd Edition. 2009. B.Magowan, Philip Owen, James Drife.
- Intrapartum intendance: NICE guideline CG190 (February 2017). Available from: [LINK].

Source: https://geekymedics.com/how-to-read-a-ctg/
0 Response to "How to Read Fetal Non Stress Test Uterin Contractions Above 120"
Post a Comment